
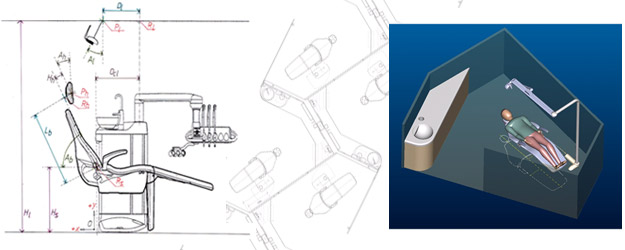
Operatory Design
- Office equipment and layout evaluations
- Dental office suite reviews
- Individual operatories
- New office architectural plan reviews
- Ergonomic Practice Assessment
- Dental Practice Risk Profile Assessment
- Dental Office Equipment / Layout Risk Assessment
- Ergonomics Training / Re-Training for Dental Health Personnel
- Recommendations for integrated intervention planning with physiatrists, physiotherapists, occupational therapists, and other health care providers
- Participation and follow-up for integrated intervention planning with physiatrists, physiotherapists, occupational therapists, and other health care providers, including reporting and coordinating with disability insurance carriers, should they wish (or require) such services

Planning Session
The Ergonomic Practice Assessment
Ergonomic Practice Assessments (EPAs) of practice ergonomics are most often requested for dentists, dental hygienists, and dental assistants as a means to determine the contribution (if any) of problematic clinical ergonomics to a particular reported discomfort, impairment, and/or disability of the clinician. The EPA will also help determine the projected role (if any) of ergonomics training/retraining or dental operatory equipment modification or adjustment for reduction of the problem and/or for rehabilitation of the individual as part of a return-to-work strategy.
The EPA proper will usually take 2-3 hours, depending upon several factors:
- the level of current relevant medical and rehabilitation records available for review prior to the EPA
- the physical resilience of the clinician
- the nature of the practice which is being evaluated (e.g., those in general practice and those in specialty practice have different ranges of activities to be evaluated.
We usually suggest that EPAs be done in the mid-morning to late morning, if possible. The clinical portion of the EPA can be completed in simulation (using specially designed simulation equipment and dentoforms) either in the clinician’s own practice operatories or at a nearby dental school or private clinic arranged for the session. It is also possible to conduct an EPA at the clinician’s office while treatment is proceeding with their own patients, provided that the range of appointed treatments provides adequate representation of the usual range of practice activities undertaken, and provided that patients agree to the observation. (Patients have always been very positive about being included when the observation by an ergonomics expert has been presented as a process of optimizing all aspects of care, and not surprisingly, patients have always given permission for their participation in such assessments, including permissions for photos and videotaping of the clinician during the treatment sessions.)
The goals of the EPA are to gain a history and profile of the clinician’s current level of application of ergonomics to the clinical dental (or dental hygiene or assisting) practice, and to determine whether any intervention and/or training might be useful for adjusting settings and/or alleviating habits which are associated with increased risks of musculoskeletal symptoms and work-related injury.
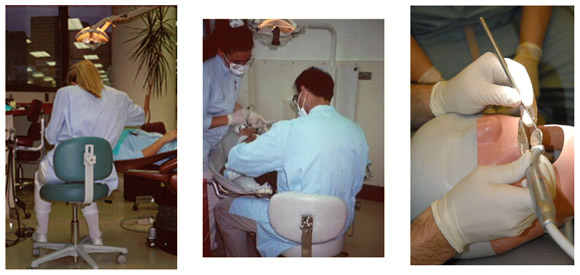
To do this we attempt to gather basic information about various aspects of the clinician’s professional training, the current (or most recent) practice settings (operatory layout, etc.), and the clinician’s current practice habits (via discussion with the clinician and via simulation exercises). We videotape certain portions of the EPA session as a part of the data-gathering. This recording is especially useful to help the clinicians (and their rehab support team) understand any problems cited in the report, and to serve as a baseline to monitor progress as the clinician moves toward comfortable return to work.
Standard industry Functional Capacity Evaluations and other work-capacity and stress-capacity measures are generalized for all types of workers and for all types of work requirements. They are useful adjunctive evaluations to help determine areas of true physical limitations which might affect clinical work, but certain aspects of clinical dental, dental hygiene, eand even dental assisting work are primarily in the micromotor domain (small muscle movement with a high degree of control but very little force).
Dental professionals by and large use very fine motor skills for which strength and stamina are not as important as the ergonomics of balance and finesse. Hence the particular need for an Ergonomic Practice Assessment. If great strength and stamina are required in modern dental practice, it is usually because the basic rules of clinical ergonomics are being violated. Such violations are quite common among practitioners, unfortunately, and the effects for an individual clinician are often obscured by the tolerance threshold of that clinician. Changes in fitness, changes in schedule, compromises of general health, and many other stress factors can alter this threshold and yield discomfort and breakdown for the clinician. One of the key strategies which can allow a motivated individual to return to practice is adjustment of the ergonomics of practice so as to optimize the thresholds for comfort and healing.
A Word to Clinicians
We are very thorough in our Ergonomic Practice Assessments (EPAs) and very conservative with our recommendations for interventions and for hardware changes in the operatories, but the reality is that such changes are occasionally required. This is especially true when the existing equipment settings disallow clinical performance with ergonomic balance regardless of how much the dental professional wants to work in balance and comfort.
There are very few specialist consultants out in the world performing such evaluations and interventions. We have enjoyed high levels of success when we can allow clinicians with ergonomic compromises to be assessed properly and to have customized interventions to allow them to return to a high level of comfortable clinical practice.
The fees associated with an EPA and associated reports will be approved by disability insurance providers, and more often than not, they will approve coverage for any recommended intervention training and follow-up. Occasionally, however, if recommendations include movement and reinstallation of any operatory hardware, or replacement of any operatory hardware, some disability insurance company reviewers may balk at funding those capital changes and improvements. In such cases, I have been called upon to provide more in-depth analysis/reporting for whomever is reviewing the proposals for such interventions.
The level of discussion depends, more than anything, upon the reviewer’s experience level with clinical ergonomics evaluations and interventions for dentists or microsurgeons (plastic surgeons, neurosurgeons, minimally invasive cardiovascular surgeons, etc.).
It is critically important to make sure that whatever time and money is being spent on physiotherapy and other conventional medical interventions, it is not being undermined or negated by ergonomic compromises in your work setting. This can be caused by limitations of the operatory equipment layouts where you are working, or from limitations in the clinician’s own level of ergonomic sophistication (which is very common among dentists and dental hygienists) or both. Until we do a proper Ergonomic Practice Assessment we don’t know.
It is impossible to know prior to an EPA what specific costs and timing for interventions (if indeed any interventions are needed) might be required as part of any ergonomic rehabilitation required. It is possible, for example, that the clinician is already optimizing an optimal workplace setting, in which case there are no interventions indicated.
Physiatrists, general work ergonomists, PTs, and OTs may make generalized observations and assessments of ergonomic compromises to postural balance, as they do for their clients in a vast array of seated (and standing) occupational configurations. Their IMEs also provide important information to complete the picture of the best way to proceed with any needed ergonomic interventions. Unfortunately, there is a tendency to presume that such generalized understanding, risk measurements, and generic recommendations for interventions (splinting and special prosthetic redesign) will suffice for those clinicians who perform in the surgical fields too. Sadly, it does not, and often only results in unnecessary and expensive delay of rehabilitation for an injured or otherwise compromised clinician.
Please feel free to contact Dr. Rucker at ErgonomicsDental.com with any questions related to any of these assessment and rehabilitation issues.
Lance M. Rucker, DDS
Professor Emeritus
3341 Flagstaff Place
Vancouver, BC
Canada
Tel: 604-433-2970
Cel: 604-803-1789
